A 74 year old male presents to a rural ED with no CT. His wife came frantic to the triage desk as he was unable to get out of his car. As Dr Poss went out to see this person, he realized that he looked unwell, was presyncopal and pre-arrest. He was put onto a stretcher and into a resuscitation area of the hospital. He is somewhat relieved by this and provides a history of 2 weeks of exertional bilateral upper shoulder pain after using a treadmill for 5 minutes or so and is relieved with rest. Yesterday the pain was more severe and today it lasted from 7-9 pm. Today the same pain came back at 3 pm as well as diaphoresis and light-headedness. he then came to the ER where nearly fainted on the drive. He has had 4 hours of pain now. Vitals are HR 82, BP 161/101, RR 16, Sats 92 RA, Temp 36.7.
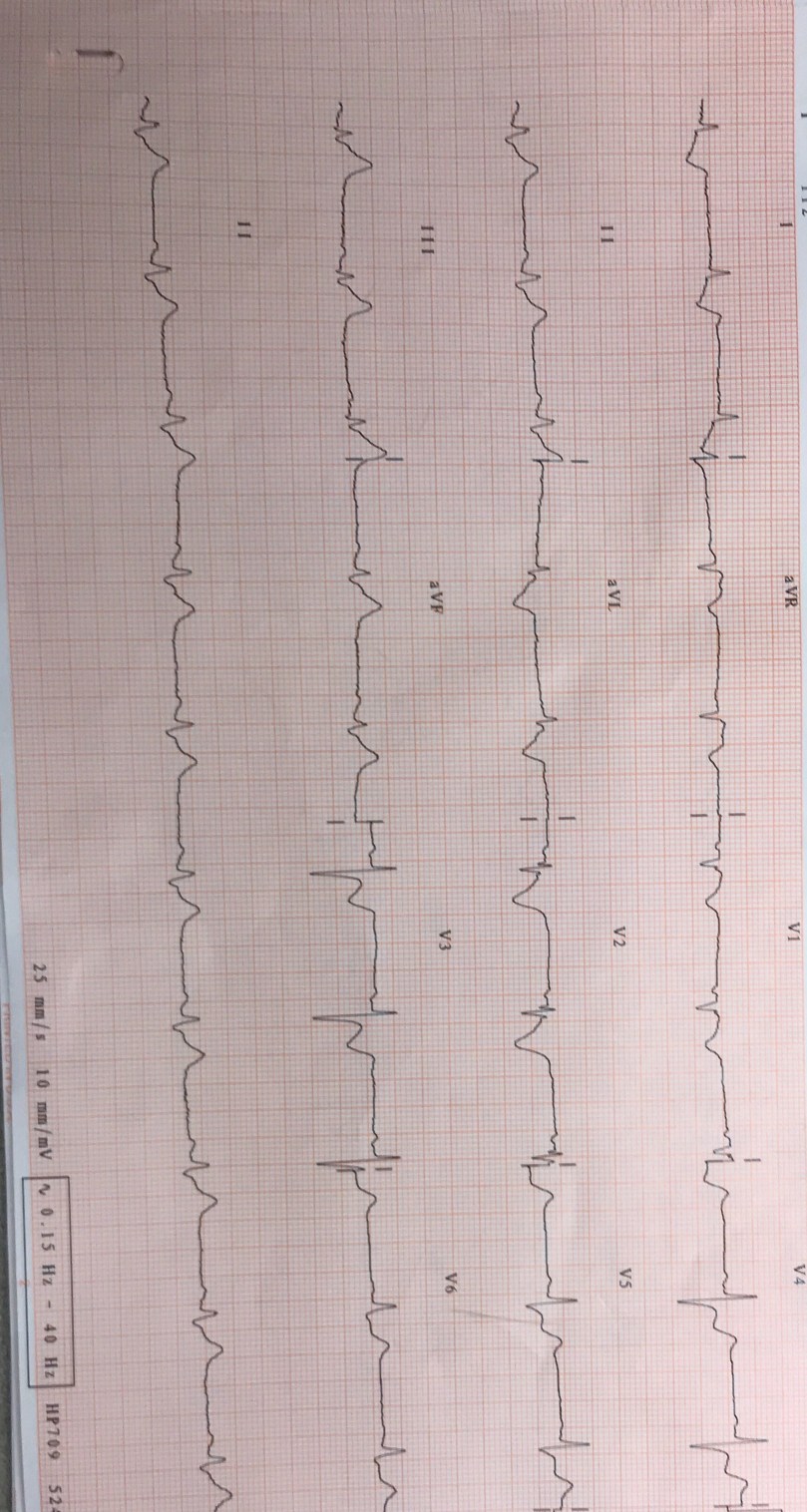
The ECG is below?
Thoughts? It is Dr Poss’s first shift here. Lab and Xray are here. There is no CT. Nearest Cath Lab is 1.5 hours away.